



Table of Contents
Nowadays, children never part with their mobile phones, and the problem of myopia (or known as nearsightedness) is becoming more prevalent. In the author’s daily work, many parents are panicky over the problem of their children’s having myopia or stronger myopia. Many parents will still hold some anachronistic concepts about the topic of “getting a new pair of myopia spectacles”, and therefore their children’s myopia problems cannot be dealt with in a timely and correct fashion. As a result, this article will focus on analyzing the 3 myths of parents about their children’s wearing myopia spectacles.
Q1. Is an automated refractor accurate?
Optometrist’s answer: Under normal circumstances, results generated from an automated refractor are only for reference and can be inaccurate. Coupling with the use of cycloplegic drugs could make autorefracting relatively more accurate.
I believe that when most parents take their children to the optician shop, they will notice an instrument that almost all spectacles stores configure – an automated refractor, also known as an autorefractor. Since its inception in the early 70’s, the automatic refracting instrument has become a great assistant for every optometrist, in evaluating the diopter or severity of refractive errors in clients. With the aid of an autorefractor, optometrists do not have to “start from scratch” while testing clients’ refractive status, saving a lot of time and effort.

Autorefractor is a good helper for optometrists. (Image source: Adobe Stock)
Nevertheless, as children and teenagers possess a high capability in accommodation, their eye ciliary muscles tend to unconsciously contract and adjust the focus when they look through an autorefractor, causing the measured power to be stronger than the actual one. For this reason, autorefractors only provide a preliminary myopia evaluation for children and adolescents, which cannot be completely accurate. Together with the use of ciliary muscle relaxation potions (collectively referred to as the cycloplegic drugs), autorefractors can more accurately measure the diopter of myopia, or astigmatism in children and adolescents, providing a more suitable benchmark for optometrists in framing the most ideal myopia control program.
Q2. At what stage do my kids have to get a pair of spectacles for myopia correction?
Optometrist’s answer: Regardless of the severity or mildness of myopia, it is better to fill a prescription as early as possible and adopt a myopia control plan.
There is a saying that if the child’s myopia does not affect his daily vision and learning, he can choose not to wear myopia spectacles, but continue to monitor its progress.
However, because the worsening of myopia involves an elongation of the eyeball, it will cause irreversible damage to the eyes, greatly increasing the probability of suffering from some severe eye ailments (such as cataracts, retinal detachment, retinal lesions, glaucoma, etc.). Therefore, once children begin to develop myopia, regardless of its severity or mildness, parents should always let your kids wear spectacles and adopt a myopia control plan as soon as possible.
The author has integrated several research results of some foreign medical literature here for the reference of interested readers.
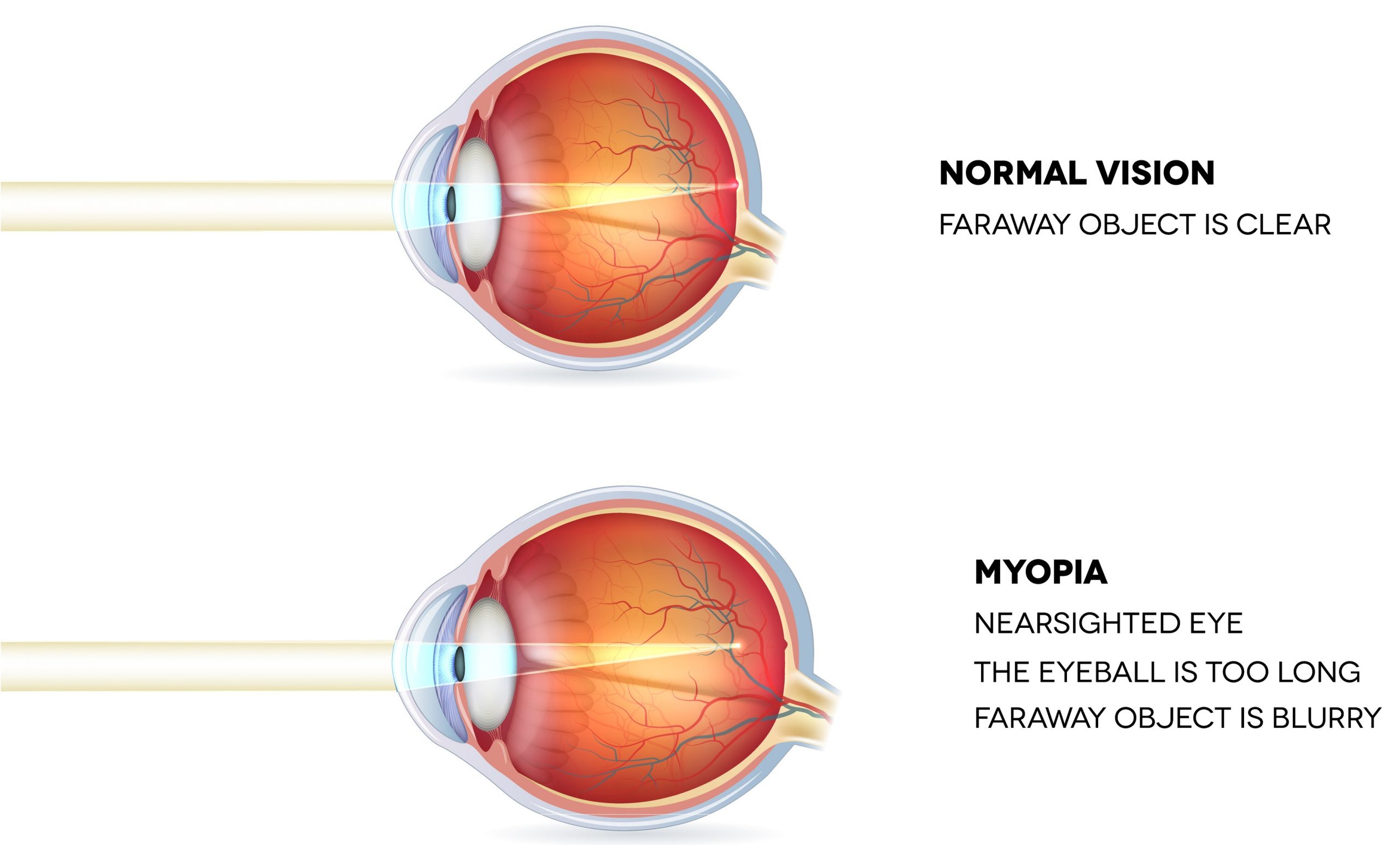 Myopia will elongate the eyeball and cause irreversible damage. (Image source: Adobe Stock)
Myopia will elongate the eyeball and cause irreversible damage. (Image source: Adobe Stock)
The deterioration of myopia can increase the probability of severe eye ailments by an exponential growth
The following is the odds ratio (OR) of some severe eye diseases in patients with different diopters of myopia.
How to read OR? Simply put, when OR is greater than 1, the probability of getting a certain kind of diseases will be multiplied. Applying to the relationship between myopia and eye diseases, OR equal to 100 indicates a 100-fold increase in probability of myopic patients suffering from a specific kind of eye ailment when compared to people without myopia.
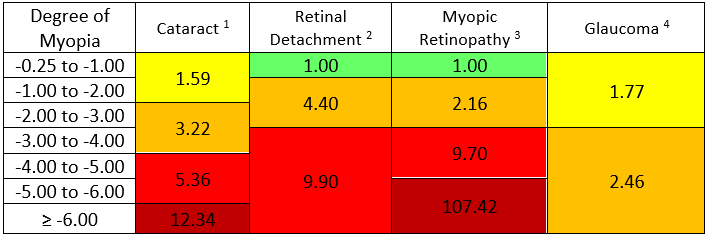
Table 1. Odds ratio (OR) of different eye diseases in patients with different diopters of myopia
As can be seen from Table 1 above, myopia is not only the problem of ‘not seeing clearly’, but also poses severe health risks and economic burden for your kids in the future. Therefore, it should always be on the top of your agenda to deal with their myopia correctly. Parents should follow the advice of the optometrists or ophthalmologists to adopt an appropriate myopia control plan for your kids as soon as possible.
Q3. Should the spectacle lens be prescribed at the exact or weaker power?
Optometrist’s answer: Children’s myopia lenses should be “prescribed accurately”, to maintain clear vision.
When filling prescription for children, it is often heard that the parents say, “The longer one wears myopia spectacles, the worsening will be the myopia situation”; “Don’t prescribe too accurate power for myopia lenses, or the myopia will deteriorate”, etc.
However, some foreign research studies showed that under-correcting myopia will not only be unable to inhibit the worsening of myopia, but also cause a counter-productive effect, and accelerate the deterioration of myopia.
As to how to “calibrate an accurate prescription”? In the optometry industry, there is a universal standard called MPMVA (Maximum Plus to Maximum Visual Acuity). Applying to the situation of myopic patients, this standard means “to achieve the best vision with the minimum myopic power”. The following is a simple example:
Kenny, who has never worn spectacles before, felt blurred when looking at the blackboard in the classroom recently. The following chart shows the visual performance of Kenny, when the optometrist gave him different myopic power:
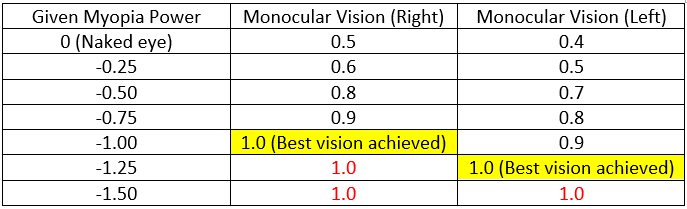
Table 2. Kenny’s monocular vision performance, when prescribed with different myopia power.
As can be seen from Table 2 above, Kenny’s right eye only needs -1.00 diopter to reach the best vision of 1.0, and giving higher power will not further improve his vision. In the same way, Kenny’s left eye only needs -1.25 diopter to achieve the best vision, so the most suitable spectacles diopter for Kenny is:
Right eye -1.00
Left eye -1.25
If myopia is over-corrected (as shown in the scarlet letters in Table 2 above), the eye ciliary muscles will continue to contract and tighten to focus at the light. Such a condition will make children prone to symptoms, such as visual fatigue and dizziness, and also not conducive to controlling the growth rate of myopia. Therefore, for children who test for myopia correction, the best policy is to prescribe a power that is just right.
5 major myopia symptoms to be on the alert for
In this era of electronics, children have more and more access to various electronic devices. However, because kids with myopia can improve their distant vision, by establishing some abnormal habits, diagnosis of myopia is often delayed. The following are the five common symptoms of myopia in children:
∞ Squinting their eyes, while looking at things
∞ Kneading their eyes often
∞ Looking too closely at things
∞ Often tilting their heads, or looking at things sideways
∞ Frequent blinking of eyes

Squinting eyes, or seeing things too closely are common symptoms of myopia. (Image source: Adobe Stock)
For the sake of your kids’ healthy eyes in the future, if parents notice the above myopia symptoms in your kids, please don’t hesitate to find an optometrist to conduct a comprehensive eye examination for your kids and adopt a myopia control plan as soon as possible.
Reference:
1. Chang, M. A., Congdon, N. G., Bykhovskaya, I., Munoz, B., & West, S. K. (2005). The association between myopia and various subtypes of lens opacity: SEE (Salisbury Eye Evaluation) project. Ophthalmology, 112(8), 1395-1401.
2. Eye Disease Case-Control Study Group (1993). Risk factors for idiopathic rhegmatogenous retinal detachment. American Journal of Epidemiology, 137(7), 749-757.
3. Vongphanit, J., Mitchell, P., & Wang, J. J. (2002). Prevalence and progression of myopic retinopathy in an older population. Ophthalmology, 109(4), 704-711.
4. Marcus, M. W., de Vries, M. M., Montolio, F. G. J., & Jansonius, N. M. (2011). Myopia as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. Ophthalmology, 118(10), 1989-1994.
5. Chung, K., Mohidin, N., & O’Leary, D. J. (2002). Undercorrection of myopia enhances rather than inhibits myopia progression. Vision research, 42(22), 2555-2559.
6. Adler, D., & Millodot, M. (2006). The possible effect of undercorrection on myopic progression in children. Clinical and Experimental Optometry, 89(5), 315-321.
7. Bayramlar, H., Gurturk, A. Y., Sari, U., & Karadag, R. (2017). Overcorrecting minus lens therapy in patients with intermittent exotropia: Should it be the first therapeutic choice? International ophthalmology, 37(2), 385-390.
Other Posts:
 【Lazy Eye】How to Prevent "Lazy Eye” and Amblyopia? Until What Age Can a Lazy Eye Be Treated?
【Lazy Eye】How to Prevent "Lazy Eye” and Amblyopia? Until What Age Can a Lazy Eye Be Treated?
Since 2019, COVID-19 has become a pandemic around ... 【Anecdotes about the History of Orthokeratology】Tracking Back to the Origin of Orthokeratology Has T...
【Anecdotes about the History of Orthokeratology】Tracking Back to the Origin of Orthokeratology Has T...
What is Ortho-K? In recent years, I believe that ...